By comparison, in the tactical and combat arenas the wounding patterns and causes of death are noticeably and dynamically different. The TCCC mnemonic MARCH that guides tactical medical care was developed and implemented specifically to address the leading preventable causes of death that have been extensively documented throughout military operations, from Mogadishu to the current actions in the Middle East and Southeast Asia.
Differences between civilian and combat trauma include the causes, setting, individuals caring for the casualties, and evacuation time (typically much longer in a combat setting). Under TCCC, tactical medicine is divided into three stages:
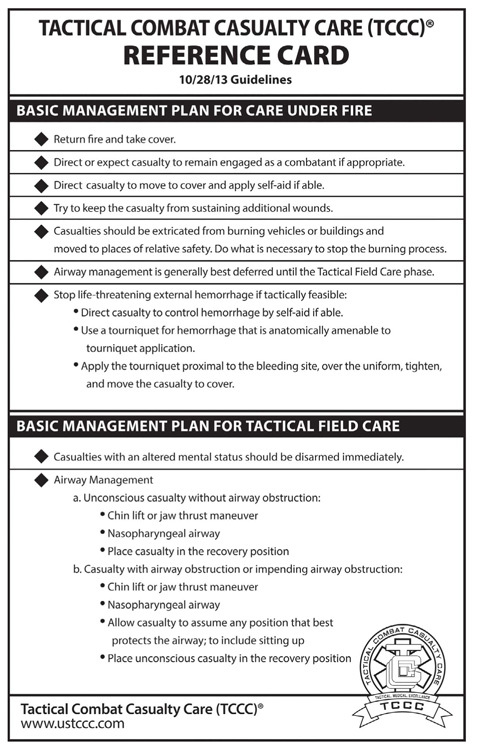
1.Care under fire. Battlefield care in the “hot zone” while under hostile fire, with only a small aid bag for equipment.
2.Tactical field care. Therapy provided once the casualty and unit are out of direct hostile fire, now in the “warm zone”; care is limited to equipment carried into the field.
3.Casualty evacuation care (CASEVAC). Treatment provided during evacuation from the immediate scene; care includes a much wider range of equipment and interventions.
It is important to remember that CLS are primarily shooters; they are not junior medics. They should be trained to provide lifesaving care as the tactical situation permits, in accordance with TCCC recommendations and guidelines. As leaders, you know what the most common causes of preventable death are and should train all members in your unit to treat these conditions. CLS training and tasks include:
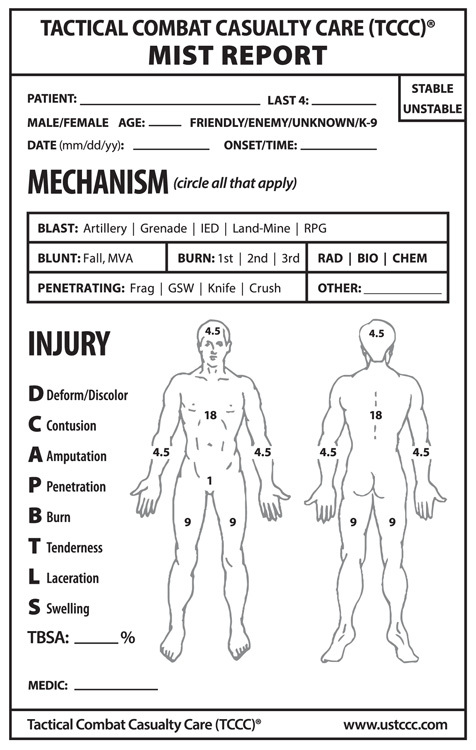
•Rapid casualty assessments.
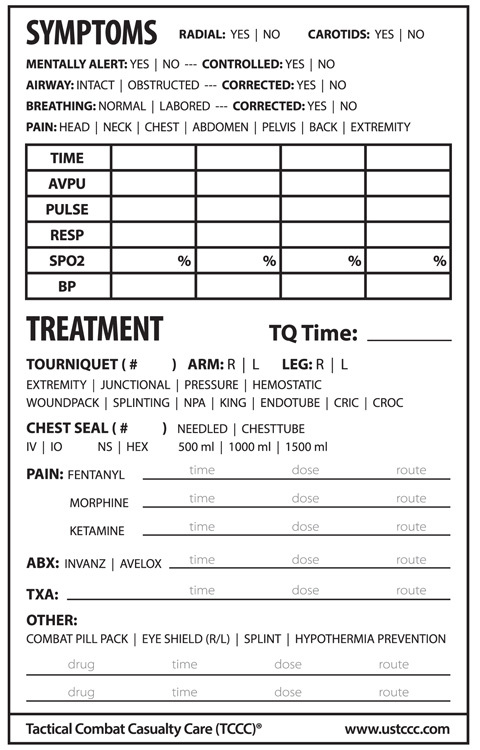
•Controlling hemorrhages.
•Treating penetrating chest trauma.
•Maintaining the airway.
•Initiating saline locks.
•Packaging casualties for transport.
•Initiating FMC.
•Initiating nine-line MEDEVAC requests.
Performance Steps
CLS should follow the following steps in order:
Step 1. Collect all applicable information needed for MEDEVAC request.
Determine the grid coordinates for the pickup site
Obtain radio frequency, call sign, and suffix
Obtain the number of patients and precedence
Determine the type of special equipment required
Determine the number and type (litter or ambulatory) of patients
Determine the security of the pickup site
Determine how the pickup site will be marked
Determine patient nationality and status
Obtain pickup site NBC contamination information (normally obtained from the senior person or medic). Note: Only included when contamination exists.
Step 2. Record the gathered medevac information using the authorized brevity codes.
Note: MEDEVAC information must be encrypted, unless transmitted over secure communication systems (see step 3b).
•Line 1: Location of pickup site.
•Line 2: Radio frequency, call sign, and suffix.
•Line 3: Number of patients by precedence.
•Line 4: Special equipment required.
•Line 5: Number of patients by type.
•Line 6: Security of pickup site.
•Line 7: Method of marking pickup site.
•Line 8: Patient nationality and status.
•Line 9: NBC contamination.
Step 3. Transmit the MEDEVAC request.
a.) Contact the unit that controls the evacuation assets:
Make proper contact with the intended receiver.
Use effective call sign and frequency assignments from the SOI.
Give the following in the clear: “I have a MEDEVAC request.” Wait one to three seconds for a response. If no response, repeat the statement.
b.) Transmit the MEDEVAC information in the proper sequence:
State all line item numbers in clear text.
The call sign and suffix (if needed) in line 2 may be transmitted in the clear.
Note: Line numbers 1–5 must always be transmitted during the initial contact with the evacuation unit. Lines 6–9 may be transmitted while the aircraft or vehicle is en route.
Follow the procedure provided in the explanation column of the MEDEVAC request format to transmit other required information.
Pronounce letters and numbers in accordance with appropriate radio telephone procedure.
Take no longer than twenty-five seconds to transmit.
End the transmission by stating “over.”
Keep the radio on and listen for additional instructions or contact from the evacuation unit.
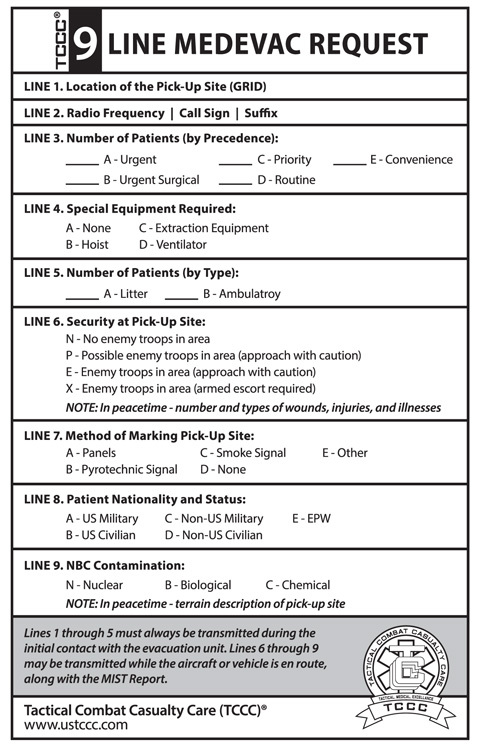
STANDARD NINE-LINE MEDEVAC REQUEST
Note: Lines 1–5 will be given when requesting MEDEVAC. Lines 6–9 can be given when A/C is en route to HLZ/PZ.
•Line 1. Six-digit grid coordinate of the pickup site
•Line 2. Radio frequency, call sign, and suffix of the requesting unit (encrypted or plain)
•Line 3. Number of patients by precedence:
Urgent—loss of life, limb, or eyesight within two hours
Urgent surgical—needs surgery to save life within two hours
Priority—loss of life, limb, or eyesight within four hours
Routine—evacuate within twenty-four hours (sick or wounded)
Convenience—for medical convenience only
•Line 4. Special equipment needed:
None
Hoist (250 feet of usable cable)
Jungle/forest penetrator
Semi-rigid litter
Stokes litter (basket type)
•Line 5. Number of patients by type:
Litter patients
Ambulatory patients
•Line 6. Broken into two situations (war and peace):
Wartime situation (pick one):
No enemy troops in the area; Possible enemy troops in the area; Enemy in the area (approach with caution); Enemy troops in the area (armed escort required)
Peacetime situation (patient information):
Vital signs; Gunshot, shrapnel, etc.; Broken bones; Illness
•Line 7. Method of marking the pickup site
•Line 8. Patient nationality and status:
US military
US civilian
Non-US military
Non-US civilian
•Line 9. Broken into two situations (war and peace):
Wartime: NBC contamination—absorbed radiation dose (RADS) of units in area/hour or type of agent used/know at PZ
Peacetime: description of the terrain around PZ to aid the pilot in locating site
Above all, stay calm. You are in charge—direct others to accomplish the mission.
COMBAT INJURIES
The following are essential tasks for tactical combat casualty care in the field.
Tourniquets
Understand the difference between mild, moderate, and severe bleeding. Know how to identify external severe bleeding (arterial bleeding).
•Direct the casualty to control hemorrhage by self-aid if possible.
•Use a tourniquet that you have had previous training on and that is properly sized to fit the extremity.
•Apply the tourniquet proximal to the bleeding, over the uniform.
•Tighten the tourniquet until bleeding has ceased, then move the casualty to cover. You may need to add an additional tourniquet above the first tourniquet to control bleeding.
Note: Do not place the tourniquet directly over the knee or elbow, holster, or cargo pocket containing items. Tourniquets should not be used if the wound is located in the neck, abdomen, groin, or armpit.
Wounded Carry Techniques
There are several different carries for injured soldiers. The conditions, manpower, and tactical situation dictate which you should use.