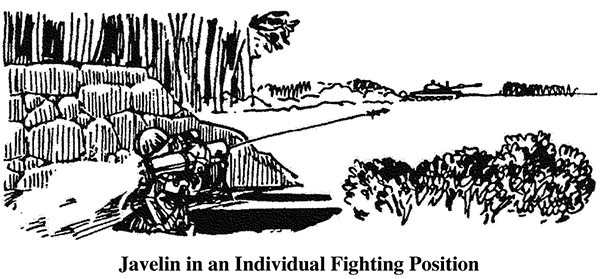
1.The gunner must keep the weapon at least 6 inches above the ground to allow room for the stabilizing fins to unfold. The hole is only waist deep to allow the gunner to move while tracking a target. Because the Javelin gunner must be above ground level, the frontal cover should be high enough to hide his head and, if possible, the backblast of the Javelin. A hole is dug in front of the position for the bipod legs.
2.When the Javelin can be fired in one direction only, the position is adjusted to provide cover and concealment from all other directions, and the Javelin should be fired to the oblique. This protects the position from frontal fire and allows engagement of the target from the flank. Both ends of the launcher must extend out over the edges of the hole.
3.Overhead cover must be built on the flanks. Cover must be large enough for the gunner, the tracker, and the missiles. Overhead cover that allows fire from underneath can be built if the backblast area is clear but must be well camouflaged.
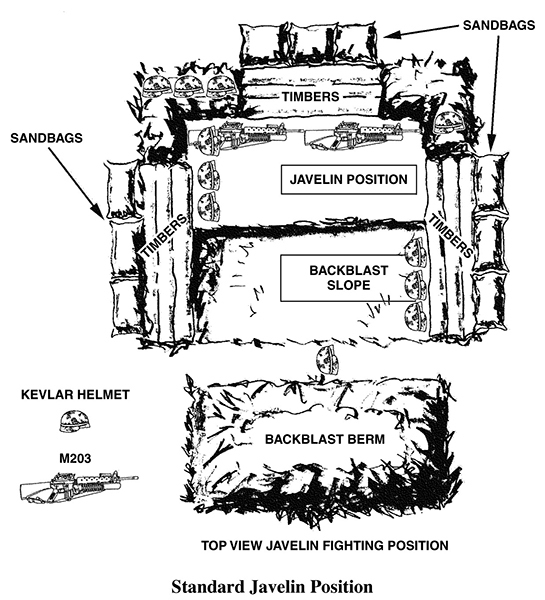
4.The Javelin is an important weapon and easy to detect; therefore, selection and preparation of alternate positions have a high priority. When preparing an alternate position, the gunner should select and improve a covered route to it so he can move to the position under fire.
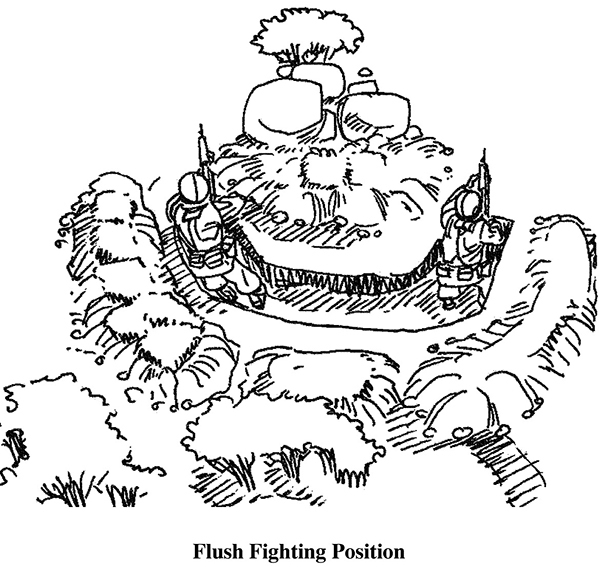
Flush Position. The flush position is a hasty position that does not provide overhead protection for the Javelin gunner during firing. The position is basically a hole dug to approximately armpit depth. Overhead cover can be prepared either to the center or the flanks of the position.
AT4 POSITION
The AT4 can be fired from infantry fighting positions. If the AT4 is to be fired from a two-soldier position, the gunner must ensure the other soldier is not in the backblast area. The soldier should assume the basic standing position, but instead of stepping forward, he leans against the back wall of the fighting position. He should ensure that the rear of the weapon extends beyond the rear of the fighting position.
MORTAR POSITIONS
The standard dug-in mortar position has three stages of construction:
1.Mortar pit.
2.Personnel shelters.
3.Ammunition bunker.
A dug-in position for 81mm or 60mm mortars is the same as for 4.2?-inch mortars, with only slight changes in dimensions. The standard mortar position should be constructed on reasonably flat ground. It can be constructed totally below, partially above, or completely above ground, depending on the time and material available and the composition of the ground.
Stage 1. After the general location is selected, the exact baseplate position is marked, and construction of the mortar pit is begun.
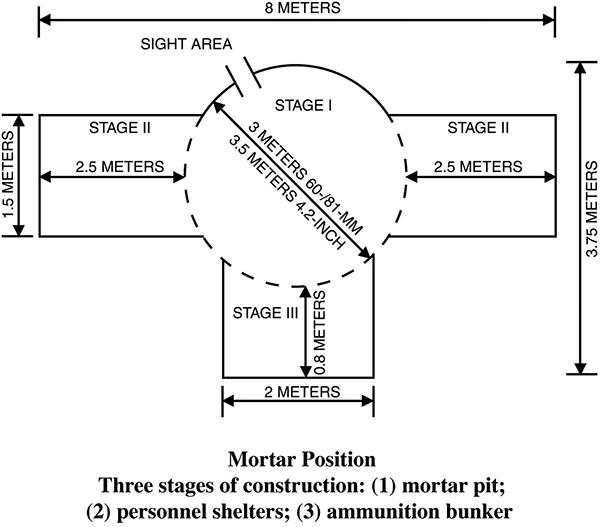
Stage 2. As soon as the mortar pit is completed, and as time allows, personnel shelters with overhead cover are constructed. Firing ports should be built into the personnel shelter and positioned as determined by assigned sectors of fire. There should be a blast barrier at least two sandbags thick separating the personnel shelters from the mortar pit.
Stage 3. If time and resources permit, ammunition bunkers are constructed. Each bunker is divided into four sections, one for each type of ammunition: white phosphorus (WP), illumination, final protective fire (FPF), and high-explosive (HE).
Camouflaging the position is done in conjunction with construction through all stages.
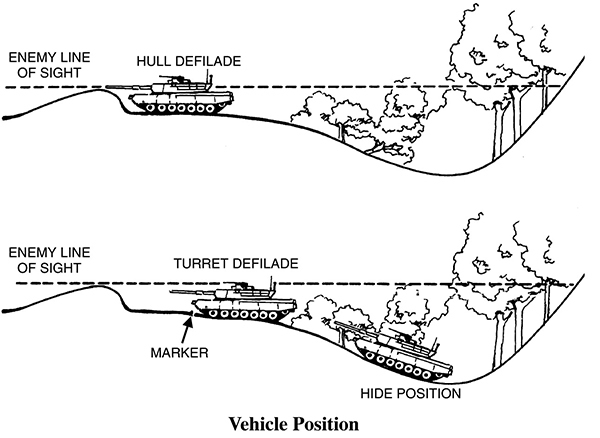
VEHICLE POSITIONS
The deliberate position is constructed in four parts: hull defilade, concealed access ramp or route, hide location, and turret defilade. The access ramp from the hide location to the hull defilade usually provides turret defilade for a vehicle at some point on the ramp. This location is marked to allow the driver to drive to it during daylight and darkness.
14
First Aid
It is important for combat leaders to understand that on today’s battlefield, first aid begins with the wounded soldier aiding themselves—self-aid should precede buddy aid if at all possible. Buddy aid is not beneficial if soldiers do not begin treating themselves first. Training in skills such as the self-application of tourniquets and hemorrhage control should be mandatory for all soldiers in any unit.
All soldiers should carry individual first aid kits (IFAK) in a predetermined area according to unit SOP and be well versed in all the contents inside the kits. IFAKs should be carried in an area that the wearer can reach in order to administer self-aid and buddy aid. The kit should not be in a location that hinders any movement needed for fighting. Further, all unit members should have training in the medical kit that is carried by the unit medic in case they have to access it themselves during an emergency.
All care should be based on the acronym MARCH—Massive bleeding, Airway, Respirations, Circulation, and Head. The science behind MARCH recognizes a particularly important principle: performing the correct intervention at the correct time in the continuum of tactical care. A medically correct intervention performed at the wrong time in combat may lead to further casualties.
DEATH IN COMBAT
The following are the leading causes of death in combat:
31 percent
Penetrating head trauma
25 percent
Surgically uncorrectable torso trauma
10 percent
Potentially correctable surgical trauma
9 percent
Exsanguination from extremity wounds
7 percent
Mutilating blast trauma
5 percent
Tension pneumothorax
1 percent
Airway problems
2 percent
Died of wounds after evacuation to an MTF, mostly from infections and complications of shock
Note: Over 2,500 soldiers died in Vietnam because of hemorrhage (bleeding) from extremity wounds (to the arm or leg), even though the soldiers had no other serious injuries.
Preventable Causes of Combat Death
Preventable causes of combat death include the following. Data is extrapolated from Vietnam to present-day Iraq and Afghanistan.
60 percent
Hemorrhage from extremity wounds
33 percent
Tension pneumothorax
6 percent
Airway obstruction, e.g. maxillofacial trauma
COMBAT LIFESAVERS AND TACTICAL COMBAT CASUALTY CARE*
Combat lifesavers (CLS) and tactical combat casualty care (TCCC) training and providers have proven to be, beyond any doubt, instrumental in dramatically increasing survivability amongst deployed troops during tactical operations (point of wounding). As a leader, ensuring that your unit is properly trained prior to deployment in both disciplines dramatically increases your potential for mission success and survivability of those in your charge. TCCC was developed to bridge the gap between civilian protocol and necessary intervention for individuals and military units deployed in tactical environments.
Historically, blunt trauma (primarily motor vehicle accidents) is the major cause of death in the civilian arena. Most medical procedures and interventions designed for use on the civilian population were based on this, hence the ABCs (airway, breathing, and circulation) of the civilian first aid algorithm. In the civilian emergency medical services (EMS) field, medical personnel are not allowed to assess the patient’s airway, breathing, and circulation until the scene is declared “safe.” This status is usually determined by local law enforcement or fire personnel and based on safety parameters that do not apply in a tactical environment among combat troops.